
Key Takeaways
- After stopping GLP-1, patients lack a clear transition plan, leading to significant weight regain.
- Weight regain often consists of fat, not muscle, increasing the risk of sarcopenic obesity.
- Five key maintenance pillars are necessary: protein intake, resistance training, body-composition monitoring, nutrient repletion, and thyroid assessment.
- The first 90 days after discontinuation are crucial for maintaining weight loss and improving body composition.
- High-risk groups, such as older adults and those with significant weight loss, require closer monitoring and intervention.
Estimated reading time: 14 minutes
You stopped the medication — or you’re about to — and nobody gave you a plan for what comes next.
Not your prescriber. Not the telehealth app. Not the pharmacy. You were titrated up, you lost the weight, and then either the prescription ended, the side effects became intolerable, or you decided you were done. And now you’re on your own.
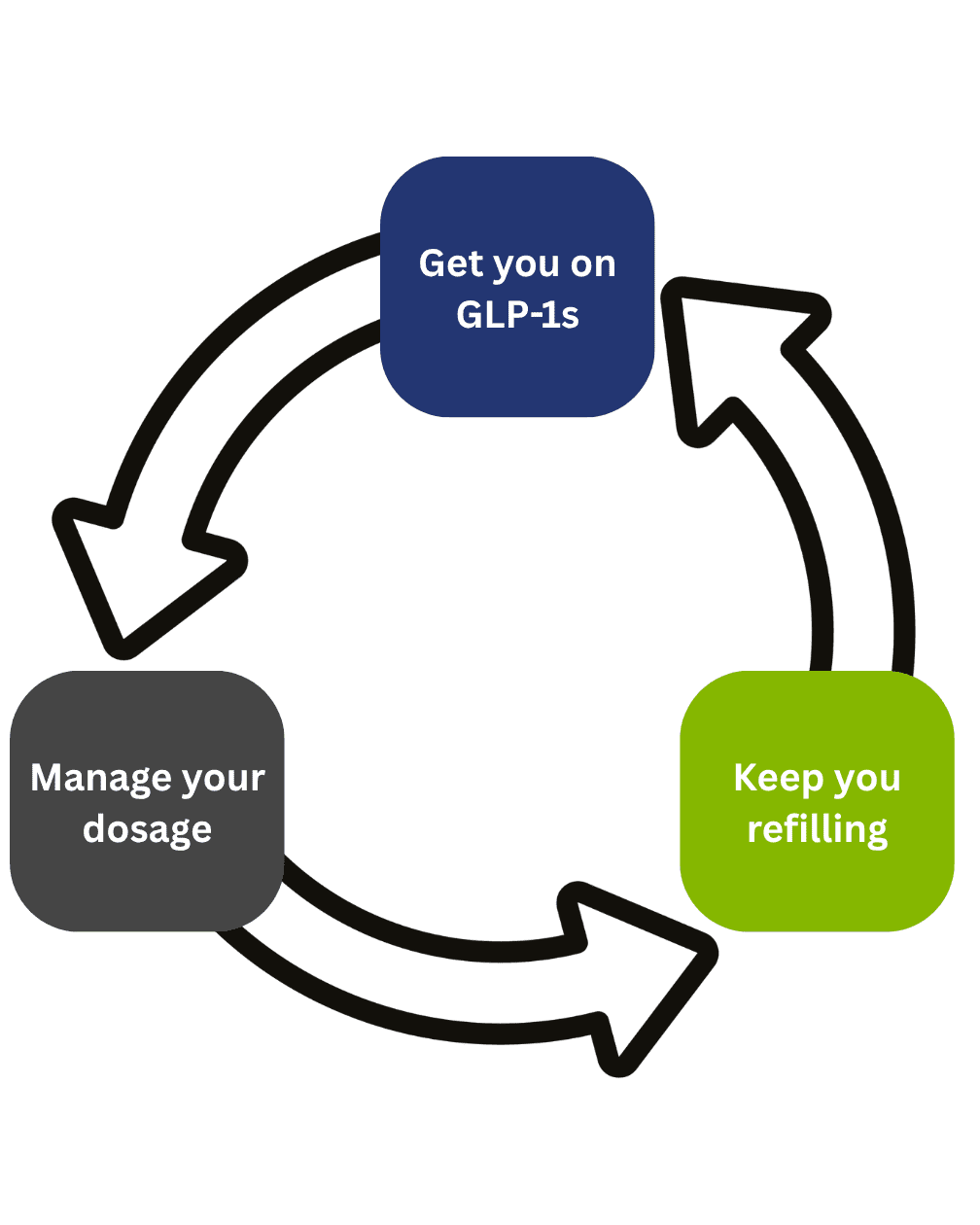
This is not a failure of willpower. It’s a failure of the model. The GLP-1 prescribing system is built to get you on the drug, manage the dose, and keep you refilling. It is not built to get you off the drug safely. There is no standard-of-care transition protocol in mainstream GLP-1 prescribing — no structured taper plan, no body-composition monitoring, no nutrient repletion schedule, no post-discontinuation follow-up. The evidence base for what to do after stopping is, as of mid-2026, remarkably thin. A 2025 systematic review and meta-analysis in eClinicalMedicine — pooling data from eight randomized trials — confirmed that weight, waist circumference, and BMI all increase significantly after GLP-1 discontinuation, and concluded that clinical guidelines need to address not just initiation and titration but discontinuation and long-term maintenance. Those guidelines don’t exist yet.
This article is a working version of what those guidelines should contain — written for the patient, not the clinician, but with enough clinical specificity that you know what to ask for and what to measure.
Why stopping without a plan leads to regain
The math is straightforward, but nobody explains it before you stop.
While you were on the medication, three things happened simultaneously. First, your appetite was pharmacologically suppressed, which means you ate significantly fewer calories — often without realizing how few. Second, because you were eating less, you almost certainly lost some lean mass (muscle) along with the fat, unless someone was actively managing your protein intake and resistance training. Third, your resting metabolic rate dropped — partly because you weigh less, and partly because your body adapted to the caloric deficit.
The STEP 1 trial extension — the most cited discontinuation data we have — showed that within one year of stopping semaglutide, participants regained approximately two-thirds of the weight they had lost. They went from a mean loss of 17.3% at week 68 to a net loss of only 5.6% at week 120. That’s not a slow drift. That’s a rapid reversal.
And here’s the part that matters most: the weight that comes back is not the same weight that left. When you lose weight on a GLP-1 without managing body composition, a significant portion of what you lose is muscle. When you regain weight after stopping, what comes back is almost entirely fat. A 2026 editorial in Cureus examining the biology of post-GLP-1 regain named this pattern explicitly: sarcopenic obesity, where you end up at a similar body weight but with a worse ratio of fat to muscle than you had before you started.
So when the medication stops:
Your appetite returns to full strength — or close to it. But you’re now eating against a body with less muscle and a slower metabolic rate. The engine is smaller, the fuel demand is lower, and the hunger is back. The weight that returns is fat, deposited on top of the muscle you already lost. You’re not back to square one. You’re behind it.
That’s the trajectory if you do nothing. It doesn’t have to be the trajectory.
The maintenance pillars
There is no single intervention that holds the line after a GLP-1. There are five, and they work together. Drop one and the others become less effective.
1. Protein — the non-negotiable foundation
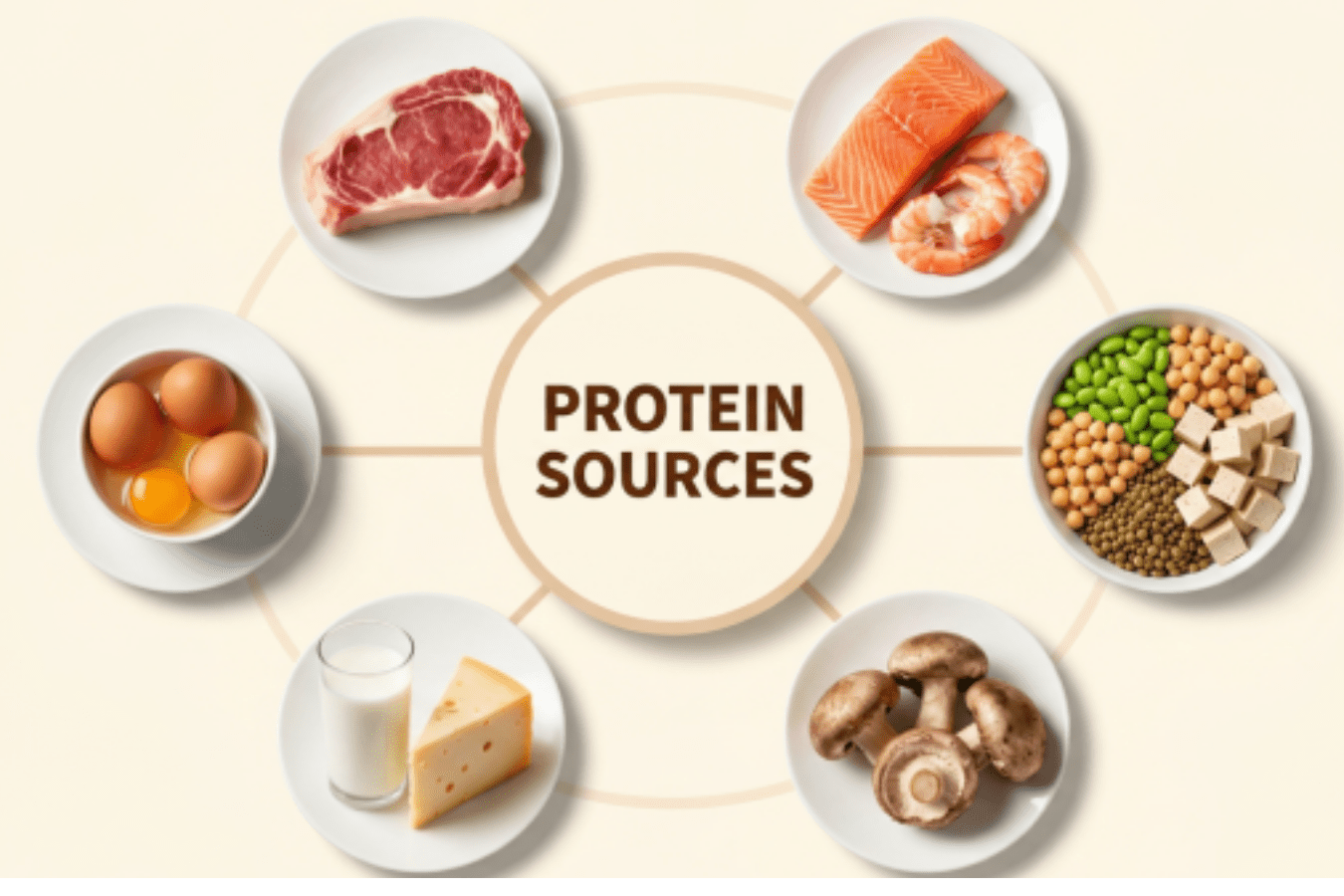
If you take nothing else from this article, take this: your protein intake after stopping a GLP-1 needs to be deliberate, tracked, and higher than you think.
While you were on the medication, appetite suppression made it hard to eat enough of anything — but protein was the first casualty. Most patients on a GLP-1 are significantly under-proteined without knowing it, because the medication makes them not hungry enough to eat the volume of food that adequate protein requires. Research drawing on bariatric surgery protocols — which face the same intake-restriction problem — suggests a range of 0.8 to 1.6 grams of protein per kilogram of body weight per day, or roughly 80 to 120 grams daily in absolute terms, as a reasonable target for preserving and rebuilding lean mass during and after major weight loss.
After stopping, this becomes even more important. You’re now trying to rebuild muscle that was lost during treatment while defending against fat regain. Protein is the substrate for both.
Practical targets: aim for a minimum of 1.2 grams of protein per kilogram of your current body weight per day, spread across at least three meals. If you weigh 170 pounds (77 kg), that’s roughly 90 to 100 grams daily. Front-load it — a protein-rich breakfast matters more than most people realize, because muscle protein synthesis is most responsive when it’s been fasted for hours.
2. Resistance training — the only thing that tells your body to keep the muscle
This is not optional. It is the single most evidence-supported intervention for preserving lean mass during weight loss and rebuilding it after.
A 2025 prospective study of 200 adults initiating GLP-1 therapy with concurrent resistance training education and individualized protein targets showed that participants lost approximately 13% of body weight but only about 3% of muscle mass at six months. That’s a dramatically better composition outcome than the unmanaged trials show. The European Association for the Study of Obesity’s Physical Activity Working Group has specifically highlighted that resistance training — not aerobic exercise — is what attenuates lean mass loss during weight-loss interventions.
After stopping the medication, resistance training serves a dual purpose: it is the primary stimulus for rebuilding lost lean mass, and it is the most metabolically protective habit you can maintain. Muscle is metabolically active tissue. Every pound of it raises your resting energy expenditure. Rebuilding it is how you bring your metabolic rate back up — and a higher metabolic rate is what gives you a buffer against regain.
The minimum effective dose: two to three sessions per week, focused on compound movements (squats, presses, rows, deadlifts or their machine equivalents), progressive in load over time. If you haven’t trained before, start with a qualified trainer. The goal is progressive overload, not exhaustion.
3. Body-composition monitoring — because the scale lies
The scale cannot tell you whether you’re losing fat or muscle. It cannot tell you whether the weight you’re regaining is fat or lean tissue. After stopping a GLP-1, the scale is worse than useless — it’s actively misleading, because early changes in body water and glycogen stores can mask fat gain or mimic muscle gain.
Body-composition testing — whether by DEXA scan or bioelectrical impedance — separates fat mass from lean mass and lets you track both over time. This is the only way to know whether what you’re doing is actually working. A stable weight on the scale can mean you’re gaining fat and losing muscle at the same rate — a terrible outcome that looks like maintenance.
Baseline scan at or near the time you stop. Follow-up at 6 weeks, 12 weeks, and then quarterly for the first year. If lean mass is stable or increasing and fat mass is stable or decreasing, you’re winning — regardless of what the scale says.
4. Nutrient repletion — refill what was quietly depleted
Months of significantly reduced caloric intake depleted more than your fat stores. The SEMALEAN study — a 2026 prospective trial of 106 patients on semaglutide — documented an initial drop in resting energy expenditure that partially recovered by month 12, along with lean mass that declined early and then stabilized. What the body-composition data doesn’t show is what was happening at the micronutrient level. When you eat dramatically less food for months, you get dramatically less of everything that food contains.
The nutrients most commonly depleted by prolonged caloric restriction include iron, ferritin, zinc, magnesium, B12, folate, vitamin D, and biotin. These aren’t abstract deficiencies — they drive the fatigue, the brain fog, the hair loss, and the flat mood that so many patients report during and after GLP-1 use. (If that sounds like you, this article explains the full picture.)
A comprehensive micronutrient panel at discontinuation tells you exactly what’s low and by how much. Repletion is targeted, not guesswork — you correct what’s actually depleted, at therapeutic doses, and retest to confirm.
5. Thyroid and metabolic check — make sure the engine is actually running
Caloric restriction downregulates thyroid function. This is well-established physiology — it’s one of your body’s adaptive responses to what it perceives as famine. The 2026 Cell Metabolism tirzepatide study confirmed that tirzepatide did not attenuate metabolic adaptation in human subjects — meaning the usual metabolic slowdown from weight loss still occurred even on the drug. When you stop the medication, you need to know whether your thyroid has downregulated and, if so, how much.
A full thyroid panel — not just TSH, but free T3, free T4, reverse T3, and thyroid antibodies — gives you the picture. If thyroid output is suppressed, supporting it is part of the recovery plan. If you skip this step, you’re trying to maintain weight loss against a metabolic rate that’s running slower than it should be.
What the first 90 days should look like
This is the critical window. The steepest weight regain after GLP-1 discontinuation happens in the first three to four months. If you can hold the line through this period with structure, the trajectory stabilizes.
Before you stop (or within the first week):
Get a body-composition scan. Run a comprehensive metabolic and micronutrient panel: CBC, CMP, full thyroid (TSH, free T3, free T4, reverse T3, antibodies), iron/ferritin, B12, folate, magnesium RBC, zinc, vitamin D, and homocysteine at minimum. If you’ve been experiencing fatigue, hair loss, or mood changes, add a full hormone panel. This is your baseline. Everything that follows is measured against it.
Start a targeted protein protocol immediately — don’t wait for lab results to eat enough protein. Minimum 1.2 g/kg/day, distributed across meals.
Weeks 1 through 4:
Begin or continue resistance training — minimum two sessions per week. If you’ve been training while on the medication, maintain or increase volume. If you haven’t, start now with a structured program.
Expect your appetite to return. This is not a sign that something is wrong — it’s the medication leaving your system. The protein and training are what keep this manageable. You are not trying to replicate the caloric restriction from the drug. You are trying to eat adequately for muscle preservation and metabolic function while your body recalibrates.
Start repletion for any deficiencies identified in your labs. Therapeutic dosing, not maintenance dosing — there’s a significant difference.
Weeks 4 through 8:
Second body-composition scan. Compare to baseline. You’re looking at lean mass trend and fat mass trend separately. If lean mass is stable or trending up, and fat mass is stable or only modestly increasing, you’re on track.
Reassess training — are loads progressing? If not, the stimulus may not be sufficient. Reassess protein — are you consistently hitting your target, or has the return of appetite shifted your eating patterns in a way that’s undermining it?
Weeks 8 through 12:
Third body-composition scan. Recheck any nutrients that were depleted at baseline — you want to see repletion, not just slow improvement.
This is also when to recheck thyroid if it was suppressed. By 12 weeks, you should have a clear picture of whether your metabolic rate is recovering, whether your lean mass is holding or rebuilding, and whether fat regain is controlled.
If the trajectory is good at 90 days, shift to quarterly monitoring for the rest of the first year.
Who needs monitoring most
Not everyone faces equal risk after stopping a GLP-1. Some populations need closer monitoring and earlier intervention:
- Adults over 60. Age-related muscle loss (sarcopenia) is already underway. Adding GLP-1-induced lean mass loss on top of it, and then stopping the drug without a rebuild plan, creates a compounding deficit. Falls, fractures, and functional decline are the downstream risks.
- Postmenopausal women. Declining estrogen already accelerates muscle and bone loss. GLP-1 treatment during this window without body-composition monitoring is a setup for sarcopenic obesity — and the metabolic consequences are harder to reverse.
- Anyone who lost more than 15% of their body weight. Greater total weight loss means greater absolute lean mass loss, greater metabolic adaptation, and a steeper regain trajectory.
- Anyone who was on the drug for more than 12 months without labs. The longer the caloric restriction, the deeper the depletion. A year of dramatically reduced intake without micronutrient monitoring is a year of accumulating deficits that won’t self-correct.
- Anyone who was not resistance training while on the medication. This is the majority of GLP-1 patients. Without the training stimulus, lean mass loss during treatment was unmitigated — meaning there’s more to rebuild, and the metabolic disadvantage is larger.
If you fall into more than one of these categories, the case for structured monitoring isn’t optional — it’s urgent.
What you can do on your own vs. when to get help
Some of this you can execute independently. Protein targets and resistance training don’t require a clinician — they require discipline and a plan. If you’ve been training and eating well while on the medication, and you have no symptoms of depletion or thyroid suppression, and you’re willing to monitor your body composition, you may be able to manage the transition on your own.
But be honest with yourself about what “manage” means. The STEP 1 extension data didn’t come from lazy or uninformed patients — it came from a clinical trial population that had structured lifestyle support while on the drug and still regained two-thirds of their weight within a year of stopping.
Get help if:
You’ve never had a body-composition scan and don’t know your fat-to-lean ratio. You’re experiencing fatigue, brain fog, hair loss, or mood changes that started during or after treatment. You don’t know your current micronutrient or thyroid status. You lost more than 15% of your body weight on the medication. You’ve already started regaining and the trajectory feels uncontrolled. You fall into one or more of the higher-risk categories above.
A functional medicine workup gives you the data — the body-composition baseline, the labs, the nutrient levels, the thyroid status — and builds the plan around what’s actually happening in your body, not a generic handout. The weight regain after stopping a GLP-1 is not inevitable. But it is the default outcome without a plan.
The bottom line
The GLP-1 did its job. It suppressed your appetite and you lost weight. But it was never designed to be the whole plan — it was designed to be one tool in what should have been a comprehensive approach to body composition, nutrition, metabolic health, and long-term maintenance. The fact that nobody built the rest of the plan around it is not your fault. It’s a gap in the model.
You can close that gap. The five pillars — protein, resistance training, body-composition monitoring, nutrient repletion, and thyroid and metabolic assessment — are the structure that gives the weight loss you achieved a chance to last. The first 90 days are the window. The data is the compass.
If you’re feeling terrible after the weight loss, there’s a reason — and it’s measurable. If the weight is already coming back, the trajectory can be changed. If the fatigue won’t let up, the workup will tell you why. If the hair is falling out, the labs will show what’s driving it.
The medication was the first chapter. This is the second one — and it matters more.
Dr. Darrell Kilcup, DC, CFMP practices functional medicine in Phoenix, Arizona. If you’ve stopped a GLP-1 and want a structured plan — body-composition baseline, labs, nutrient repletion, and a maintenance protocol built around your data — you can start as a new patient or call (602) 864-0304 with questions. Out of state? The lab workup, nutrition plan, and training prescription can be done remotely — call to ask about phone and video visits.
Related reading:
- Why You Feel Terrible After Losing Weight on a GLP-1
- Weight Coming Back After Stopping Ozempic
- Hair Loss on Ozempic and Wegovy
- Ozempic Fatigue That Won’t Go Away
- Adrenal Fatigue can make you FAT, TIRED, LIBIDO-LESS, CONSTIPATED AND SICK
- The KEY to Weight Loss
- Causes of Chronic Fatigue | A Functional Medicine Perspective
 In Office
In Office
 By Phone
By Phone





