
Key Takeaways
- Stopping GLP-1 medications like Ozempic often leads to rapid weight regain, as clinical trials have shown that most patients regain a significant portion of lost weight once they discontinue use.
- This weight regain occurs due to biological responses, as the body’s appetite and metabolic functions revert to their pre-treatment state after stopping the medication.
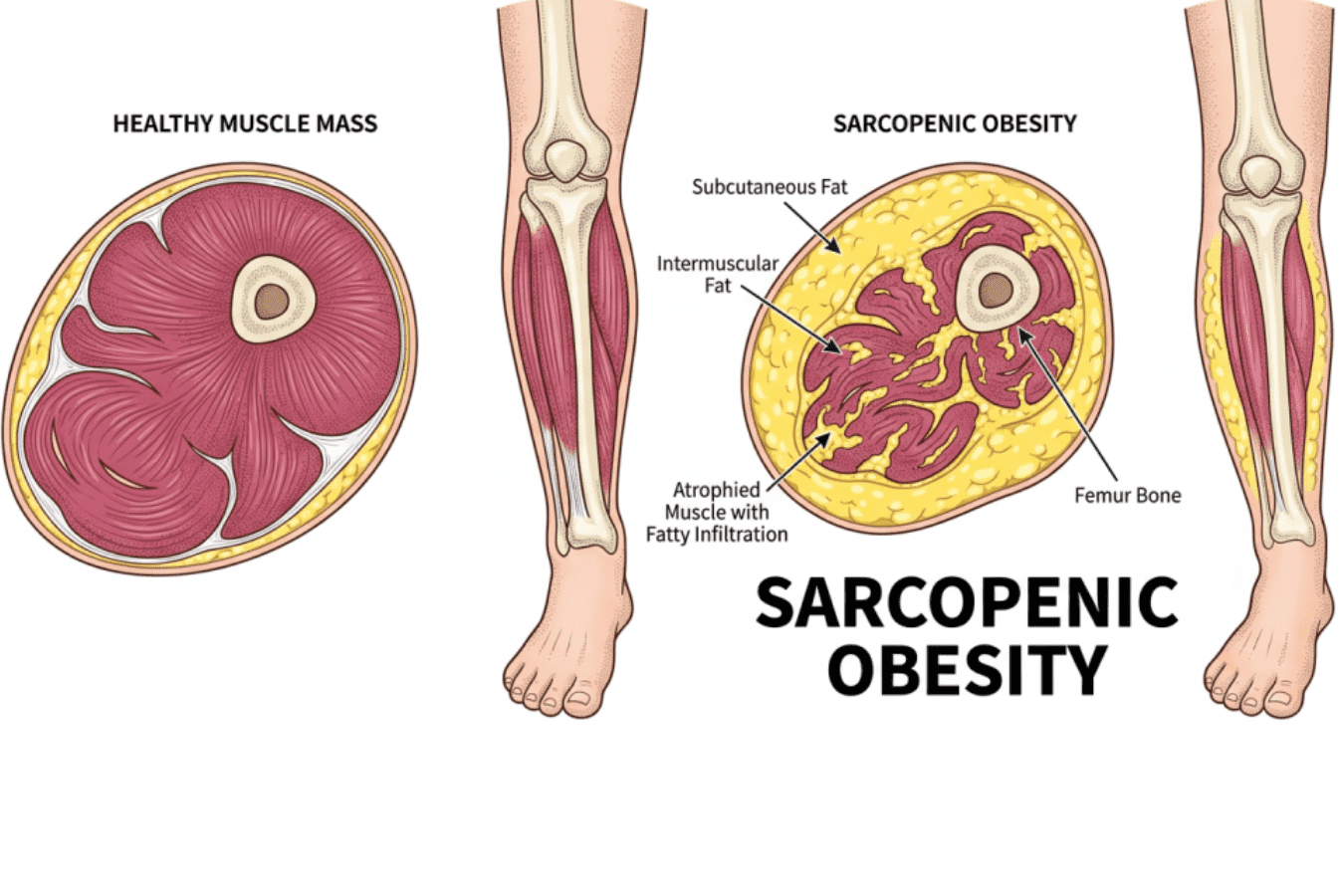
- Patients typically lose a mix of fat and lean mass while on GLP-1s, but regain fat predominantly when they stop, leading to a risk of sarcopenic obesity.
- Prescribers often fail to provide a post-treatment plan, leaving patients without guidance on how to manage their weight regain effectively.
- Implementing body-composition monitoring, adequate protein intake, resistance training, and metabolic assessments can help manage the trajectory of weight coming back after stopping Ozempic.
Estimated reading time: 11 minutes
Weight Coming Back After Stopping Ozempic? Here’s What’s Actually Happening.
You stopped the medication. The weight is coming back. And it’s coming back fast.
You did what you were supposed to do. You took the drug, you lost the weight, and at some point — maybe by choice, maybe because of cost, maybe because your doctor changed course — you stopped. And now the scale is climbing and you can feel your body changing and nobody warned you this would happen.
You are not failing. You are not weak. You are experiencing exactly what the clinical trials predicted — and what your prescriber probably never explained.
I’m Dr. Darrell Kilcup. I’ve been practicing functional medicine in Phoenix for over 35 years, and right now I’m seeing more patients walk through my door with this exact story than almost any other. Here’s what the research actually says, why it’s happening, and what you can do about it.
The research is clear: weight comes back after you stop
This is not a “some people” problem. It is a nearly universal finding across every major trial.
The landmark STEP 1 extension study followed patients for a year after they stopped semaglutide (Wegovy). On average, participants regained two-thirds of the weight they had lost during treatment. The cardiometabolic improvements — blood pressure, blood sugar, cholesterol — reversed along with it.
The SURMOUNT-4 trial told the same story for tirzepatide (Zepbound). A post hoc analysis found that within one year of stopping, 82% of participants had regained more than a quarter of their lost weight. More than half regained 50% or more.
And in March 2026, a systematic review and meta-regression published in eClinicalMedicine pulled together 48 studies and modeled the trajectory mathematically: at one year after stopping a GLP-1, patients regained roughly 60% of their lost weight. The model estimated that regain eventually plateaus — but at about 75% of the weight that was lost.
Let that sink in. If you lost 40 pounds on the drug, the average trajectory puts you at regaining 30 of them.
Real-world data tells a similar story. A large Danish population study of 77,310 adults found that 52% of people who started semaglutide for weight loss stopped within the first year — and the regain data from the trial extensions applies directly to that population.
None of this means the drugs don’t work. They work well while you’re on them. The problem is what happens when you stop — and the fact that almost nobody is given a plan for that moment.
Why the weight comes back: it’s biology, not willpower
When you take a GLP-1 medication, it does several things at once. It suppresses your appetite centrally — in your brain. It slows gastric emptying so food stays in your stomach longer. It changes the hormonal signaling that drives hunger and satiety.
When the drug leaves your system, every one of those effects reverses. Your appetite comes back — often stronger than before, because your body has been in a caloric deficit for months and its weight-defense systems are fully activated.
This is not psychological. Your body has a set point — a weight range it defends through hormonal and metabolic feedback loops. The 2025 AACE obesity guidelines put it plainly: body fat is biologically defended, and weight regain after stopping a GLP-1 occurs because the therapeutic suppression of appetite and satiety regulation is gone.
You are not losing a battle of willpower. Your biology is doing exactly what it evolved to do — defend its energy stores. The drug was overriding that system. Without it, the system reasserts itself.
The part nobody talks about: what comes back is not what left
Here is where it gets worse, and where I need you to pay close attention.
When you lost weight on a GLP-1, you did not lose only fat. Research shows that up to 25–40% of total weight lost on these medications can be lean mass — muscle, bone mineral density, connective tissue. The exact proportion depends on the drug, the dose, how long you were on it, and whether you did anything to protect muscle while you were losing weight.
Now here’s the critical part: when the weight comes back after you stop, it comes back overwhelmingly as fat.
A 2026 preclinical study from Penn Medicine, published in the Journal of Clinical Investigation Insight, found exactly this pattern: weight lost on semaglutide included a mix of roughly 40% muscle and 60% fat, but weight regained after stopping was almost exclusively fat. The study also found that each cycle of stopping and restarting the drug produced diminishing returns — less weight loss each time, with an increasingly unfavorable body composition.
A review published in Cureus in February 2026 framed this as the central risk: sarcopenic obesity — where you end up at the same weight as before, but with less muscle and more fat. That is a worse metabolic position than where you started.
And a mini-review from ScienceDirect examining this question in older adults noted that weight cycling — losing weight, regaining it, losing again — has been specifically linked to lower lean mass, reduced muscle strength, and accelerated age-related muscle loss. Each cycle makes the next one harder.
This is what I mean when I say nobody gave you a plan. It’s not just that the weight comes back. It’s that the weight that comes back is the wrong kind of weight — and the weight you lost included tissue your body needs and cannot easily replace on its own.
Why your prescriber didn’t prepare you for this
I don’t say this to blame anyone. Most GLP-1 prescribing today happens through telehealth platforms, primary care offices, or med spas that are set up to do one thing: write the prescription and manage the dose. They are not set up for what comes after.
The clinical trial infrastructure behind these drugs was designed to prove they cause weight loss. It proved that convincingly. But the STEP and SURMOUNT trials also showed clearly that when the drug stops, the weight returns — and the medical system has not built anything to catch that.
There is no standard-of-care protocol for GLP-1 discontinuation. There is no required body-composition monitoring. There is no off-ramp plan built into the prescription. You get the drug, you lose the weight, and when you stop — by choice or by circumstance — you are on your own.
That gap is what I address in my practice.
What actually works: the three things that change the trajectory
I’m not going to pretend there’s a simple trick. There isn’t. But the research points to three interventions that consistently separate the people who hold their results from the people who don’t.
1. Body-composition monitoring — not just a scale
The scale cannot tell you what you’re gaining back. Ten pounds of fat and ten pounds of muscle weigh the same but mean completely different things for your metabolism, your function, and your long-term health.
Body-composition testing — whether by DEXA scan, bioelectrical impedance, or another validated method — is the only way to know whether you’re holding lean mass or losing ground. If you were never tracked during treatment, we start by establishing where you are now. If you were tracked, we compare.
This is the anchor metric. Without it, you are guessing.
2. Protein and resistance training — the non-negotiables
Muscle does not rebuild itself passively. It requires two inputs: adequate protein and progressive resistance training. Period.
Most patients coming off a GLP-1 are eating far too little protein for their current situation. Their appetite was suppressed for months. Their dietary patterns shifted toward small portions and calorie avoidance. The habits that helped them lose weight are now working against them — because they need to build, and building requires fuel.
A protein target built for your body weight, your activity level, and your recovery goals is one of the first things we set. Combined with a structured resistance program — not “try to exercise more” but an actual progression plan — this is what protects and rebuilds lean mass.
3. Metabolic and hormonal assessment
Months of caloric restriction change things. Your thyroid may have downregulated. Your resting metabolic rate may have dropped. Nutrient depletions — iron, vitamin D, B12, magnesium — may be dragging your energy and recovery down in ways that make everything harder.
A functional medicine workup looks at what actually happened metabolically while you were on the drug and gives us a map for what needs to be corrected. This is not guesswork. It’s labs, it’s data, and it’s a protocol built around what the numbers say. [Related: Why You Feel Terrible After Losing Weight on a GLP-1]
If you already know this is what you need — body-composition data, labs, a real nutrition and training plan — you can start as a new patient here or call (602) 864-0304 and we’ll walk you through how it works. If you want to keep reading first, I’ll explain the timeline below.
The window matters
Here’s the part I want to be direct about: the sooner you act after stopping, the better your trajectory.
The eClinicalMedicine meta-regression found that regain follows a predictable curve — fastest in the first 23 weeks, then decelerating. That means the first six months after discontinuation are the critical intervention window. The metabolic defense systems are most active during that period, and the decisions you make then have the largest effect on where you end up a year later.
If you’re reading this and you stopped your GLP-1 two weeks ago or two months ago, you are in the window. If you stopped six months ago and the weight is climbing, you are still in a position to change the trajectory — but the sooner the better.
And if you’re still on the medication and thinking about stopping, this is the time to build the plan — before you need it.
What this looks like at our clinic
I don’t prescribe GLP-1s. I don’t manage your prescription. What I do is everything that should be happening around the prescription — and everything that matters after it ends.
Here’s what happens when a post-GLP-1 patient comes in.
First visit: we find out where you actually are. That means body-composition testing — not a scale, not BMI, but an actual measurement of how much of your current weight is fat, how much is lean mass, and how that compares to where you need to be. It also means a full panel of functional labs: thyroid, metabolic markers, iron, vitamin D, B12, magnesium, hormones — everything that months of suppressed appetite and caloric restriction can quietly deplete. By the time you leave this visit, we have a real picture. Not a guess. Not a symptom checklist. Data.
Then we build the plan around the data. A protein target calibrated to your body weight, your activity level, and the specific goal of rebuilding lean mass — not a generic handout. A structured resistance-training prescription — the single most evidence-supported intervention for protecting and restoring muscle after weight loss. And a targeted supplement and nutrient-repletion protocol based on what your labs actually show, not what’s trendy.
We track it over time. Body-composition scans at regular intervals so you can see lean mass holding or rebuilding, fat percentage stabilizing, and metabolic rate recovering. This is what accountability looks like when it’s built on measurement instead of motivation.
For local patients in Phoenix, I also offer red-light therapy (photobiomodulation) and hyperbaric oxygen — both of which support tissue recovery, muscle repair, and the kind of cellular-level restoration that matters after prolonged caloric restriction.
If you’re out of state, the lab workup, nutrition coaching, and training prescription can all be done remotely. Body-composition scans can be arranged locally and results sent to us.
The weight coming back is not the end of the story. It’s the beginning of a different conversation — one that should have started before you ever stopped the drug.
Dr. Darrell Kilcup, DC, CFMP practices functional medicine in Phoenix, Arizona. If the weight is coming back after stopping a GLP-1 and you want a real plan — not another prescription — you can start as a new patient or call (602) 864-0304 if you have questions. Out of state? The lab workup, nutrition plan, and training prescription can be done remotely — call the office to ask about phone and video visits.
Related reading:
 In Office
In Office
 By Phone
By Phone





